Before you give birth, your cervix has to be ready
At the beginning of your birthing journey is an open cervix—but this does not happen to all women automatically. And that’s completely common. In that case, we just need to help the cervix to soften and dilate. This is called “cervical ripening”.
A relaxed, dilated cervix is just one aspect of inducing labour. In short, labour induction is completing your pregnancy by natural birth. This process involves several important steps.
Induction of labour can take anywhere from several hours to a few days. Studies show around 40–70% of DILAPAN-S inductions deliver within 24 hours of arriving at the hospital. It depends on both the clinical protocol used and how the process goes on.
A relaxed, dilated cervix is just one aspect of inducing labour. In short, labour induction is completing your pregnancy by natural birth. This process involves several important steps.
Induction of labour can take anywhere from several hours to a few days. Studies show around 40–70% of DILAPAN-S inductions deliver within 24 hours of arriving at the hospital. It depends on both the clinical protocol used and how the process goes on.
Inductions are more frequent than you may think. In fact, 1 in 3 pregnant women are induced.
Induction of labour process
Here are the 5 typical steps of induction. Actually, you may only need a couple of these to go into labour. Every childbirth is unique and may vary for everyone. However, one of the essential steps is the cervical ripening—this is when DILAPAN-S is used.
step 1
Assesing your cervix
step 2
Preparing your cervix
step 3
Breaking your waters
step 4
Starting your contractions
step 5
Meeting your baby
Still unsure about what cervical ripening means?
Imagine that you are the baby and you find yourself in a room with a closed door. The room in this story is a uterus, and the closed door is a cervix. If a big bouncer—contractions—tries to throw you out through the closed door, the outcome won’t be ideal.
First, we have to open the door, so that you can leave safely and comfortably. DILAPAN-S can help open the door for you.
Why choose DILAPAN-S?
Non-pharmacological—no drugs
Gentle and gradual—less pain during the ripening
Proven safety profile—possibility of outpatient ripening
Freedom and comfort—you can walk, shower, relax, or sleep
Valued by mothers—induced women evaluate DILAPAN-S as superior to other cervical ripening products
What to expect with DILAPAN-S
Designed to support the natural ripening process, opening your cervix gently over time.
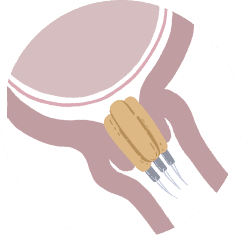
1. Insertion
Your clinician will carefully place small DILAPAN-S dilators (usually 3–5) into your cervix.
2. Relax
The DILAPAN-S dilators will gradually expand, gently helping your cervix to soften and dilate.
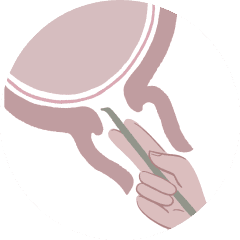
3. Removal
Your clinician will usually remove DILAPAN-S within 12–24 hours. After this, your cervix should be soft, stretchy and dilated.
We recommend to discuss the method of labour induction with your healthcare provider. Being properly educated may help you make informed, confident decisions.
We’ve put together a short guide on how to approach the discussion with your clinician.
You can carry on with your
day up until the Big Moment
With DILAPAN-S inserted, you can go about your usual business—so sit back, take the best nap of your life, read a book, do some gentle yoga or binge-watch your favourite show.
Simply relax and focus on the coming baby. Depending on your specific situation, your clinician may even send you home with the dilators in place. Just make sure to avoid baths and sexual intercourse.
How do healthcare providers evaluate your Bishop score?
Bishop score explained
What you need to know about Apgar score
The importance of skin-to-skin: More than a hug
What happens right after your baby is born?
FAQs about Dilapan-S and induction of labour
Discover DILAPAN-S: A non-pharmacological gentle option for cervical ripening
All you need to know
Induced labour may be a time of new challenges and even concern. We want to make sure that you have all the information you need to feel confident and calm. So, let’s talk about induction of labour and DILAPAN-S—listen to all of the frequently asked questions answered in a single video.